Why the Braden Scale Is Accurate but Doesn’t Work—and the Very Simple Thing You Can Do About It


Pressure injuries remain one of the most expensive and frustrating problems in healthcare. Every hospital knows the stakes. Patients suffer, caregivers feel the strain, and costs mount quickly. Yet many...

As of 2016, it was estimated that 2.5million people contract a pressure injury. Over 60,000 Die from pressure injury related complications From 2016 to present, the rate of pressure...
We dug into the latest research on pressure injuries—and the numbers tell a sobering story. The familiar ‘2.5 million cases per year’ is still widely cited, but the true burden is...
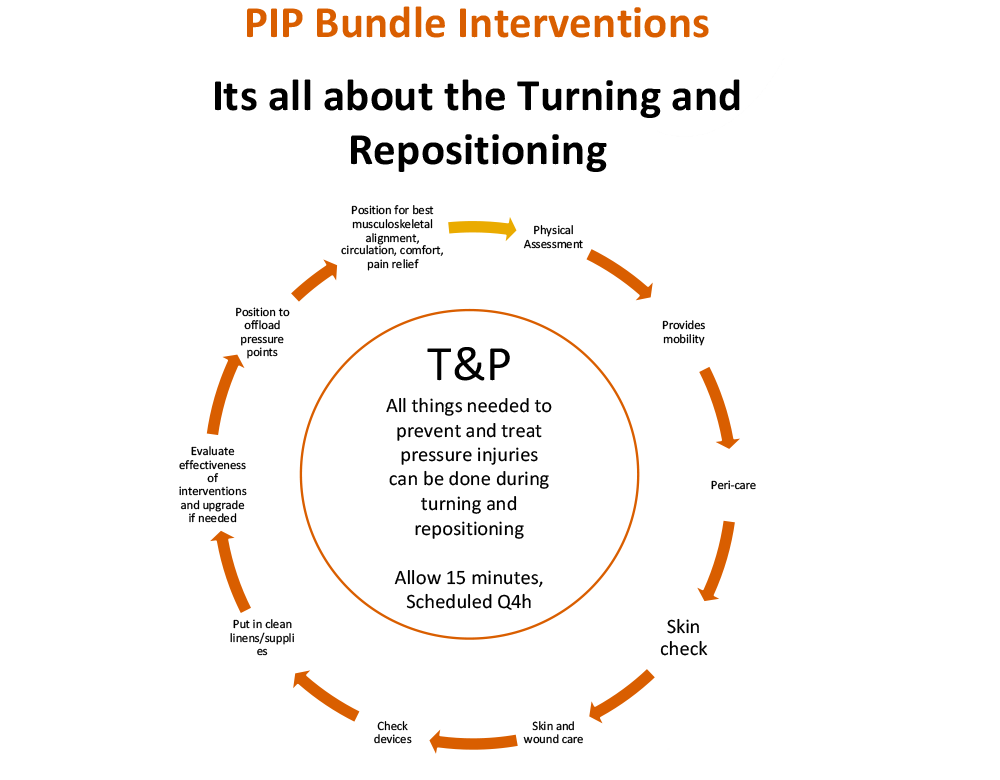
Turning and repositioning (T&P) is not just about moving a patient—it is the cornerstone of pressure injury prevention and treatment. When performed intentionally, T&P becomes a bundled 15- minute intervention...
“If he has a bedsore, it's generally not the fault of the disease, but of the nursing” - Florence Nightingale, 1859 Although pressure injuries have been happening to people since...

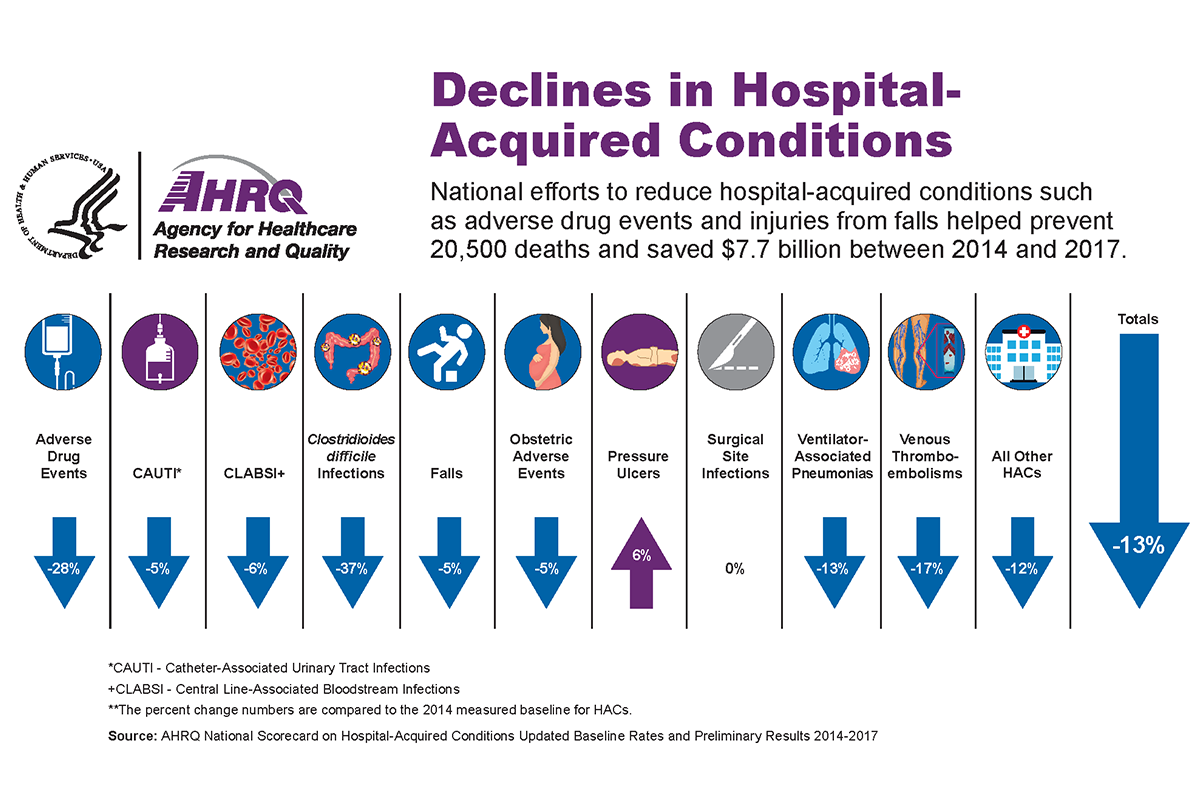
Pressure injuries remain one of the most preventable hospital harms—so why do they keep happening? Unlike many hospital-acquired conditions (HACs), such as central line–associated bloodstream infections (CLABSIs) or catheter-associated urinary...

Remember, when it comes to stopping pressure ulcer development and healing, The #1 goal is removing pressure. It can be tricky to get the pressure off the lower backside, especially when...
Many people have asked me if it is ‘legal’ to ask the hospital/skilled nursing facility/care home where my loved one is staying to use the Bedsore Rescue Backbone Positioning Cushion?...
Canadian hospitals in the Toronto area are stepping up their commitment to stop pressure injuries.Jewell Nursing Solutions and Plexxus Shared Service Organization of Toronto have secured a purchasing agreement for...
And how these myths affect HAPI rates, costs, and outcomes By Gwen Jewell, Clinical Nurse II, BSN, CWS Wound Care Pressure Injury Prevention Keywords: Pressure Injury, Pressure Injury Prevention, Turning...

If we want to realize genuine improvement in the quality of the pressure injury prevention and treatment we deliver, we cannot start with Electronic Health Records or technology driven approaches...
My Scope of Practice: Take a Load Off By Barbara Zeiger, originally published in OWM Journal May 5th, 2017 Gwen Jewell, RN, BSN, CWS, often asks herself why she is so...

Turn Therapy is to assist and provide movement for a person who is mobility impaired, especially to turn from side to side and elevate the heels. Turn Therapy is essential care...

Remember, when it comes to reducing pressure ulcers, Removing Pressure is the #1 goal. It can be tricky to get the pressure off the back, especially when a person is...
Really when you think about it, if you have to support a supine person just so, far enough to lift him off his sacrum but not so far as to...