And how these myths affect HAPI rates, costs, and outcomes
By Gwen Jewell, Clinical Nurse II, BSN, CWS Wound Care Pressure Injury Prevention
Keywords: Pressure Injury, Pressure Injury Prevention, Turning and Repositioning, 30 Degree Lateral turn, Pressure Injury Incidence, Pressure Injury Prevalence, Pressure Ulcers
“Beware of the half truth. You may have gotten hold of the wrong half “
– Anonymous
They are called Pressure Injuries for a reason. Complex as the etiology and treatment of pressure injuries are, one thing is common to all pressure injuries: Too much pressure for too long.
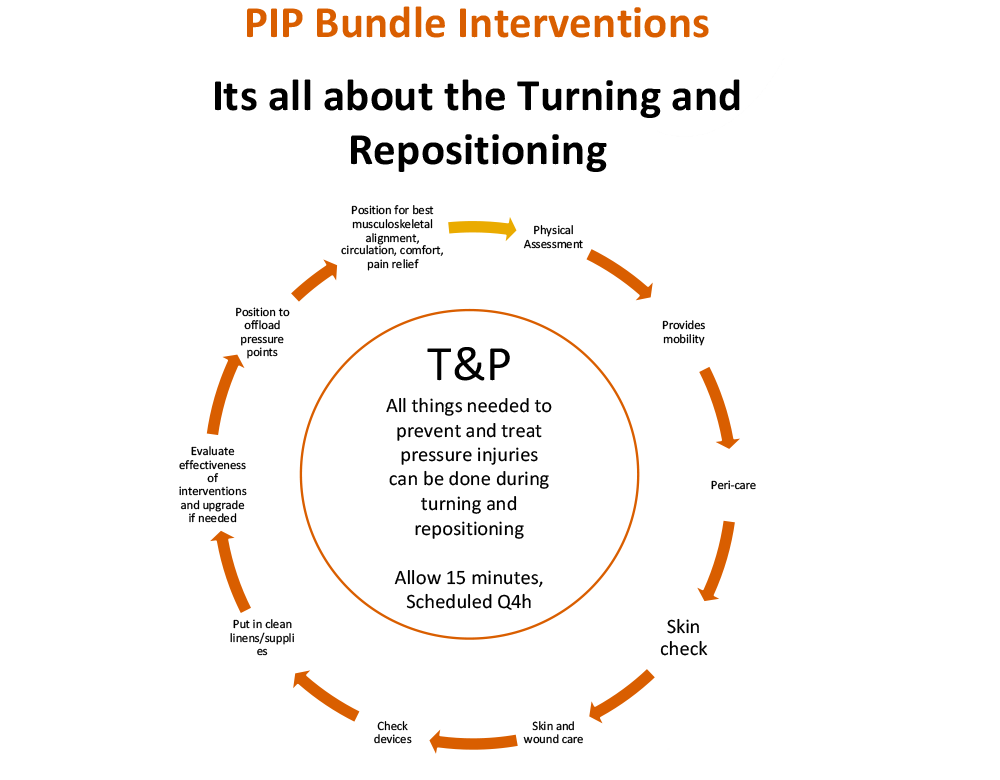
Turning and repositioning has been the go-to solution to relieve pressure for as long as pressure injuries have been around.
As time-honored and respected as turning and repositioning is, it’s a wonder there is still so much confusion about it. Everybody believes in it, but no one really thinks about exactly what they believe. And when it comes to reality, the line between the truth and the myths is more blurry than a windshield with an oil spill on it.
As a wound care and acute care bedside nurse, I have studied the turning and repositioning of the bed bound patient exhaustively. From patient’s body mechanics to the nursing process to equipment design and use. I have learned there are many very important aspects of turning and repositioning that are often overlooked or misunderstood.
Not only can these misconceptions lead to a failure to achieve our most important goal of preventing Hospital-Acquired, Facility Acquired and Community-Acquired Pressure Injuries, but these myths can and do encumber our ability to sustain effective prevention policies and programs.
A more clear understanding of this critical intervention can profoundly improve the success in preventing injuries, especially hospital acquired pressure injuries (HAPI) and facility acquired pressure injuries.
The reader might identify and agree with my assessments, or maybe feel a little provoked to dispute my assertions. Either way, I hope this commentary will challenge all who share similar aspirations to stop pressure injuries to pause, reflect and step out of the proverbial “paradigm rules” box to think about how we may better approach this most important nursing intervention:
Myth # 1. Turning and repositioning prevents pressure injuries
It’s not so much a myth as it is myth-leading.
Of course turning and repositioning HELPS prevent pressure injuries. Better said, if a patient who is at high risk for developing a pressure injury is never turned and repositioned, that person is likely to get a pressure injury. As such, turning and repositioning is a no-brainer for hospitals and skilled nursing facilities. Since the days of Florence Nightingale, tried and true, turning and repositioning has been standard operating procedure for all hospitals and nursing facilities.
The myth part is, its not turning and repositioning itself prevents a Pressure injury. It is what we are trying to accomplish accomplish when we turn and reposition. The most important being to remove pressure and support the patient in a position of sustained pressure relief from vulnerable skin and underlying tissues, especially the sacrum, coccyx, buttocks and heels. It is removing pressure that prevents pressure injuries. If a person is turned and repositioned without pressure removal, the maneuver will not prevent a pressure injury. We should be saying “Pressure relief prevents pressure injuries”
At first glance, the terminology we use may seem irrelevant. But the problem is, the protocol causes caregivers to focus just on getting the turning and repositioning done. We are not trained to make sure the patient is supported in a position of sustained pressure relief. We have protocols for turning and repositioning, but we dont have processes evaluate if it’s done correctly. And the truth is, much of the time the patient enjoys true pressure relief for less than 15 minutes. Because either we did not position correctly in the first place, or the support device we used to support the patient did not ‘hold’, or the patient did not stay in the turned position.
Turning and repositioning can prevent pressure injuries. But only if it is done correctly.
Myth # 2: We are required to turn and reposition patients every two hours. Its the law.
The “must turn q2h” is perhaps the most pervasive and misunderstood myth in all of pressure injury prevention history. The Q2h paradigm is the big half truth that locks up everything.
First of all, turning every 2 hours is not a rule or a law. Its a paradigm. The National Pressure Injury Advisory Panel states that turning and repositioning frequency should be tailored according the the needs of the patient. Not every patient needs to be turned every two hours. Again, the implication is that if a patient is not turned every 2 hours, all at risk patients would get a pressure injury. If that was true, our overall pressure injury rates would be sky high, because in reality most facilities do not have the staff to keep up with that kind of pace.
The 2 hour timeline goes way back to Florence Nightingale. Florence determined the 2-hour turn frequency time interval not because she had evidence or even collected data about it, but because it took her about 2 hours to round on her patients.
It wasn’t for another 80 years or so before it came up again. In the early 1950s when the famous neurologist Dr. Ludwig Guttman suggested this same interval for spinal cord injured patients. Again, he did not base his suggestion on any known information, but rather more as a proclamation: “In my opinion, we should turn everybody at least every 2 hours.”
The Q2h rule is confusing at the least, and counter productive at best. It could be true, but it could also not be true. If everyone was turned every two hours, and if they were supported correctly in that turned position so there was no pressure on their bony prominences, and if the patient remained in that correct pressure relieved position for the entire 2 hours, and if all the many other risk factors were well controlled, maybe that person would not get a pressure injury. But maybe they would anyway because of some other internal or external risk factor(s). But maybe if they were turned every 4 hours, correctly, they would not get a pressure injury. But maybe they would get one anyway because of some other risk factor that could not be controlled. And so on, and so forth.
To date there is still no study out there that has come up with conclusive data that turning every two hours works best. We still don’t know what the optimal frequency of turning and repositioning should be. The reason being there are too many other factors that cause pressure injury.
The idea that there can be one, same treatment or certain time period that applies to all patients and all circumstances is unrealistic. We cannot make broad sweeping assumptions what is best for every patient because every patient is different, every circumstance is different.
What we need to do is standardize the way our caregivers measure risk, perform interventions and assess the results of their efforts. In other words, we have to teach our caregivers how to do it right.
Myth # 3: Mandating turning every two hours is the safest way to go
“You cannot solve a problem with the same consciousness that created it.”
– Albert Einstein
No myth bothers me more than this one. Don’t get me wrong. If I had my way, every hospital and skilled nursing facility would have designated staff whose sole responsibility is to go bed to bed to make sure everybody who needs it is mobilized, turned & repositioned on a schedule according to that patients needs.
Its when we just mandate Q2h protocols just to “keep it simple” or because we think it’s going to keep us out of trouble we are fooling ourselves.
Turning and repositioning is highly labor intensive, time consuming and expensive. Unless facilities are able to financially support adequate staffing, where 2 caregivers can devote at least 10 to 15 minutes to each and every patient every 2 hours while managing all the many many other competing priorities required of caregivers, it is unrealistic to believe that all patients can be turned anywhere near this often.
Besides all that, lets not forget its not the right frequency for every patient. Even when there is enough staff to turn every two hours, there is evidence that waking a patient every 2 hours to turn him/her can lead delay recovery.
Perhaps the greatest crime of perpetuating this myth is when we send our patients and the loved ones who will be caring for him/her home with these instructions. We are telling them to keep up with a physically demanding and unnecessary pace, day and night. We don’t teach him/her exactly how to do it.
We can either perpetually bang our caregivers’ heads (and backs) against the 2 hour turn clock and pray for better results. Or we can incorporate pressure injury prevention care into the fabric of the nurses and aids daily practice, tailored to the patients specific needs, as we do for other care interventions.
“What it takes to prevent pressure injuries is a commitment (and training) of all the staff to all the core elements of pressure injury prevention”
– Margaret Heale (link).
Myth #4 Turning and Repositioning is simple and easy.
The complexity of turning and repositioning continues to go mostly unrecognized in healthcare.
There are many variables and co-morbidities that lead to a pressure injury. But peel back the onion layers of any pressure injury incident and somewhere in there you will always find the problem of getting pressure relief. More specifically, the problem of turning, positioning and supporting a person so that there is effective pressure relief.
Turning and repositioning is rarely easy. A short list of potential complications to turning and repositioning includes, but is not limited to the patient being physically very heavy, the patient refusing or pushing against the turn due to fear, pain, dementia, discomfort or many other reasons. He/she may be too unstable to be turned, be too restless or tend to shift back on their back soon after being positioned. They may have muscleskeletal or neurological conditions that make supporting a side turn difficult. The list goes on and on. There are so many reasons why turning can be difficult it could make your head spin. But suffice to say only the concept of T&P may be simple. The practice can be quite difficult..
In fields of healthcare such as lift team training may train turning and repositioning in some detail. But I find that for the most part most caregiver training is limited and over simplified. There is usually a brief statement about supporting a 30 degrees lateral angles, floating and lifting without sliding, and how to use lift equipment.
There is virtually zero training about the principals of physical therapy, physiology, ergonomics and biomechanics. Even physical therapy education rarely go over turning and repositioning the bed bound patient. Without exception, all trainings tell caregivers that simple pillows are adequate to support a person in a pressure relieve position, despite clear evidence to the contrary.
Turning is a science, a therapy, and a complex medical intervention. It is critically important not just for pressure injury prevention, but also serves many physiologic functions. Doing it right without the caregiver or patient injury (including pressure injury) takes practice, experience, skill and good equipment. If we are going to get better at preventing pressure injuries, we have to get smarter about turning and repositioning. We can do this by studying and understanding the science of turning and repositioning.
Caregiver training should include safe patient handling and ergonomic safety for both the patient and the caregiver. The focus should be on techniques to minimize stress and maximize musculoskeletal alignment and distributed support so that patient is stable and comfortable, and pressure reduction and circulation and microclimate are optimized.
Most importantly, we need to stop pretending that we don’t need equipment designed for the purpose. I think it’s fair to say that we have to stop pretending that pillows can do the job. We spend billions of dollars each year treating pressure injuries and paying caregivers to turn and reposition over and over again just so that we don’t have to spend thousands on good pressure injury prevention support equipment.
Doing the same thing over and over again expecting different results is not just expensive, its the definition of insanity.
Looking forward
Myths about turning may be ubiquitous, but they do not have be limiting. We have come a long way in the science of pressure injury prevention. Once we are able to integrate the nursing process with science, technology and reality, I believe we can stop pressure injuries. As Dr. Joyce Black says, “The trick is to get the pressure off.”
REFERENCES
1. Bergstrom N., Horn S.D., Rapp M.P., Stern A., Barrett R., Watkiss M. Turning for Ulcer Reduction (TURN): A multisite randomized clinical trial in nursing homes. J Am Geriatr Soc. 2013 Oct: 61(10) 1705-13
2. Borgueta, E.M. Musafar, A. Elk, K.R, Fay, M. S.T.O.P (Synchronized Turning of Patients) Reduction of Hospital Acquired Pressure Injury in the Intensive Care Unit. CCRN Annual Conference 2018 Poster Presentation.
3. Brindle C.T., Creehan S., Black, J. Zimmerman D. The VCU Pressure Ulcer Summit: Collaboration to Operationalize Hospital-Acquired Pressure Ulcer Prevention Best Practice Recommendations. Journal of Wound, Ostomy & Continence Nursing: July/ August 2015; 42(4) 331-37
4. Bush T.R., Leitkam S., Aurino M., Cooper A., Basson M.D. A Comparison of Pressure Mapping Between Two Pressure-Reducing Methods for the Sacral Region. Journal of Wound, Ostomy and Continence Nursing 2015;42(4):338-345
5. Buss I., Halfens R., Abu-Saad H. The Most Effective Time Interval For Repositioning Subjects At Risk of Pressure Sore Development. Rehabilitation Nursing 2002;27(2):59-66
6. Defloor T., De Bacquer D., Grypdonck M.H. The Effect of Various Combinations of Turning and Pressure Reducing Devices on the Incidence of Pressure Ulcers. Int J Nurs Study; 2005;42(1):37-46
7. Gillespie B.M, Chaboyer W.P, McInnes E., Kent B., Whitty J.A., Thalib L. Repositioning for pressure ulcer prevention in adults. Cochrane Database of Systematic Reviews 2014, Issue
8. Art. No.: CD009958 8. Heale, M. Repositioning and Pressure Injury Prevention: The Devil is in the Detail. WoundSource; 2018; https://www.woundsource.com
9. Krapfl L.A., Gray M. Does Regular Repositioning Prevent Pressure Ulcers?. Journal of Wound, Ostomy and Continence Nursing 2008;35(6):571-7
10. Kennerly, S, Yap, T The Role of Manual Patient Turning in Prevention Hospital Acquired Conditions. A white paper for Leaf Healthcare, www.leafhealthcare.com 2016
11. Meehan M. National Pressure Ulcer Prevalence Survey. Adv Wound Care 1994; 7:27-37
12. National Pressure Ulcer Advisory Panel & European Pressure Ulcer Advisory Panel. Prevention and Treatment of Pressure Ulcers, Clinical Practice Guidelines. NPUAP & EPIAP. Washington, 2009
13. Nixon J., Nelson E.A., Cranny G., Iglesias C.P., Hawkins K., Cullum N.A. et al. Pressure Relieving Support Surfaces: A Randomized Evaluation. Health Technology Assessment 2006; 10(22): 1-180
14. Peterson M.J., Schwab W., van Oosrom J.H., Gravenstein N., Caruso L.J. Effects of Turning On Skin-Bed Interface Pressures in Healthy Adults. J Adv Nurs. 2010 Jul;66(7):1556-64
15. Pickham, D., Berte, N. Pihulic, M. Valdez, A. Mayer, B. Desai, M. Effect of a Wearable Patient Sensor On Care Delivery For Preventing Pressure Injuries in Acutely Ill adults: A pragmatic randomized clinical trial (LS-HAPI study). Intl Journal of Nursing Studies 80 (2018) 12-19.
16. Powers J. Two Methods for Turning and Positioning and the Effect on Pressure Ulcer Development. J Wound Ostomy Continence Nurs. 2016;43(1):46-5
17. Reddy M., Gill S., Rochon P. Preventing Pressure Ulcers: A Systematic Review. JAMA 2006; 296(8): 974-84
18. Shardell, M. et al. Frequent manual repositioning and incidence of pressure ulcers among bedbound elderly hip fracture patients Wound Repair Regen. 2011 January ; 19(1): 10–18.
19. Thomas, D. R. Prevention and Treatment of Pressure Ulcers, J Am Med Dire Assoc 2006; 7: 46-59
20. Vanderwee K., Grypdonck M., Defloor T. Effectiveness of an Alternating Pressure Air Mattress for the Prevention of Pressure Ulcers. Age and Aging 2005; 34: 261-7
21. Wong V., Skin Blood Flow Response To 2-hour Repositioning in Long-Term Care Residents. A pilot study. J Wound Ostomy Continence Nurs. 2011;38(5):529-537
22. Yap, T.L, Cox, J.Turning and Repositioning Science and Implementation. 2018 National Pressure Ulcer Advisory Panel Conference Lecture Presentation.
23. Lavine, J. New Research Challenges “Q2H” Turning Standard for Pressure Injury Prevention. 2013, http://jmlevinemd.com/new-research-challenges-q2h-turning-standard-forpressure-ulcer-prevention/